banner
Evolution of the Radiologist
Radiologists were once responsible for nearly every step in the imaging process: interpreting plain films, adjusting images, and sometimes even overseeing the scans themselves. In the early days, this was manageable. Imaging volumes were low, and the studies were relatively simple. But as CT and MRI technology advanced, that changed rapidly. Modern scanners generate thousands of images per exam, and clinical teams now expect detailed reformats and 3D reconstructions to guide increasingly complex interventions.
To keep pace, the radiologist’s role began to shift. Starting in the late 1970s and continuing through the 1980s, as CT and MRI became standard clinical tools, scan acquisition was delegated to trained technologists. This allowed radiologists to focus more on interpretation. Today, a similar shift is happening with image data. The demand for advanced visualization, such as segmentation, planar reconstruction, and quantitative measurements, has created a new workload that is no longer sustainable for radiologists alone. In response, a new role has emerged: the 3D Imaging Technologist. Just as image acquisition was offloaded decades ago, the technical work of image processing is now becoming its own profession, supporting efficiency and focus in modern imaging departments.
Learn more about the evolution of a radiologist’s role here.
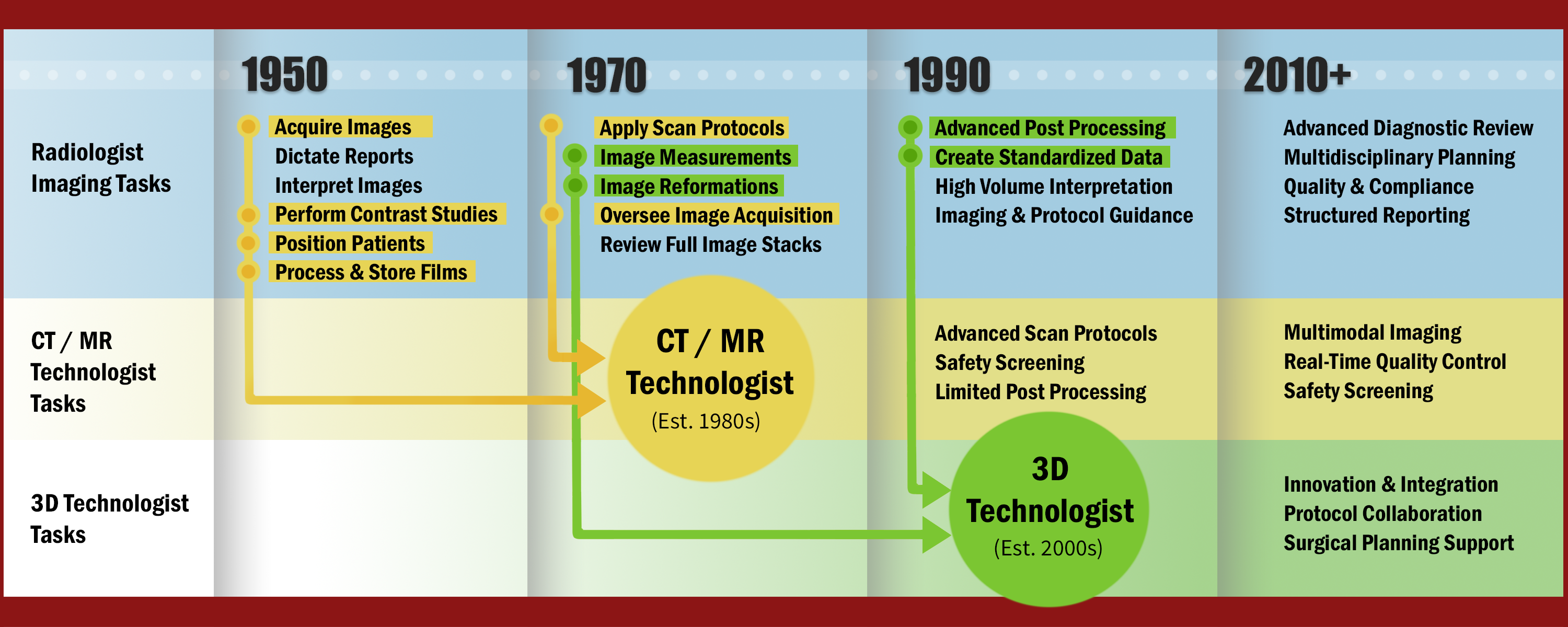
Figure A: A timeline displaying how the radiologist’s imaging job duties have been delegated over time to other, less high-skill high-pressure roles.
Why 3D Labs Exist
As 3D imaging technologists took on more of the technical workload, hospitals began organizing that work into formal units called 3D labs. By centralizing this work, 3D labs ensure consistency, streamline collaboration, and allow imaging teams to respond efficiently to clinical needs. Radiologists and referring clinicians can submit specific requests or highlight structures of interest, making the outputs more targeted and clinically relevant. Many labs also support innovation by testing new visualization tools, integrating AI applications, and developing in-house solutions to improve workflow. By taking on this technical burden, 3D labs allow radiologists to focus on interpretation, consultation, and other tasks that require their medical expertise.
Figure B: Graphed aortic measurements overtime are important for correctly timing cardiac interventions. Measurements like these can be obtained and graphed by technologists, supplying the final report to the radiologist for review.
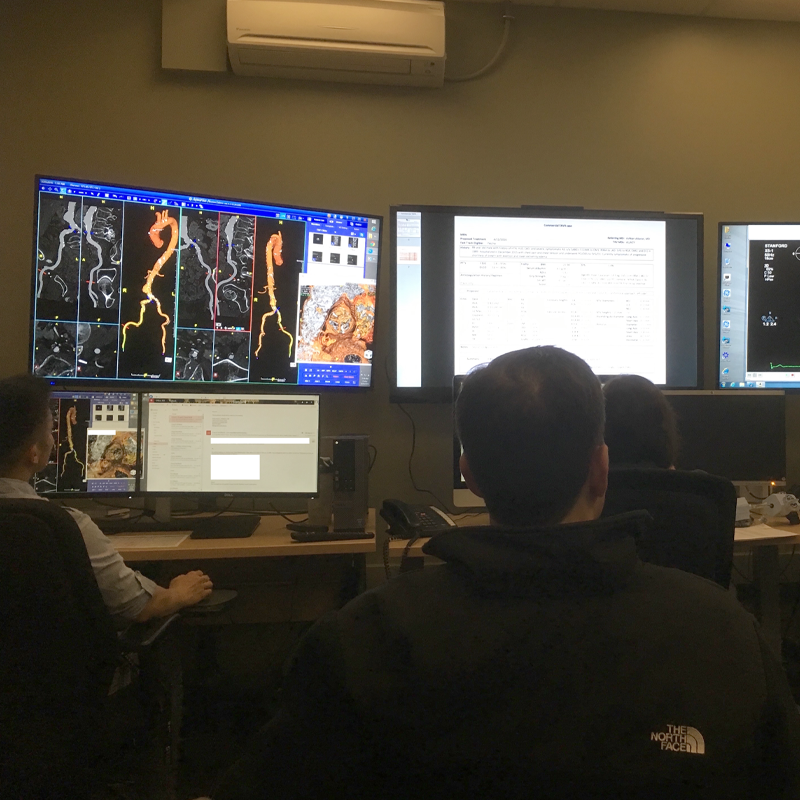
Figure C:TAVR meetings bring together specialists from multiple fields to review imaging collaboratively. The images are generated and adjusted in real time by 3D Lab members, allowing everyone to interpret the anatomy and contribute to the decision-making.
Figure D: neurosurgical guidance blurb
Technical Labor at Lower Cost
Most tasks performed in a 3D lab, such as segmentation, reformats, and volume rendering, are technical rather than diagnostic. They can be handled by technologists trained in anatomy, imaging principles, and specialized software. Typically, the educational path for a 3D Imaging Technologist is the same as for CT or MR technologists. It involves a two-year associate or four-year bachelor’s degree in radiologic sciences, followed by clinical experience and certification. This stands in contrast to the 13 or more years of education and training required to become a radiologist.
This difference in training and licensure allows 3D labs to assign non-interpretive tasks to mid-level professionals at significantly lower cost. The model mirrors what already exists in image acquisition, where technologists handle the technical execution and radiologists focus on diagnostic interpretation. Extending that division of labor into post-processing helps manage imaging volume while preserving radiologist expertise for high-level clinical decision-making.
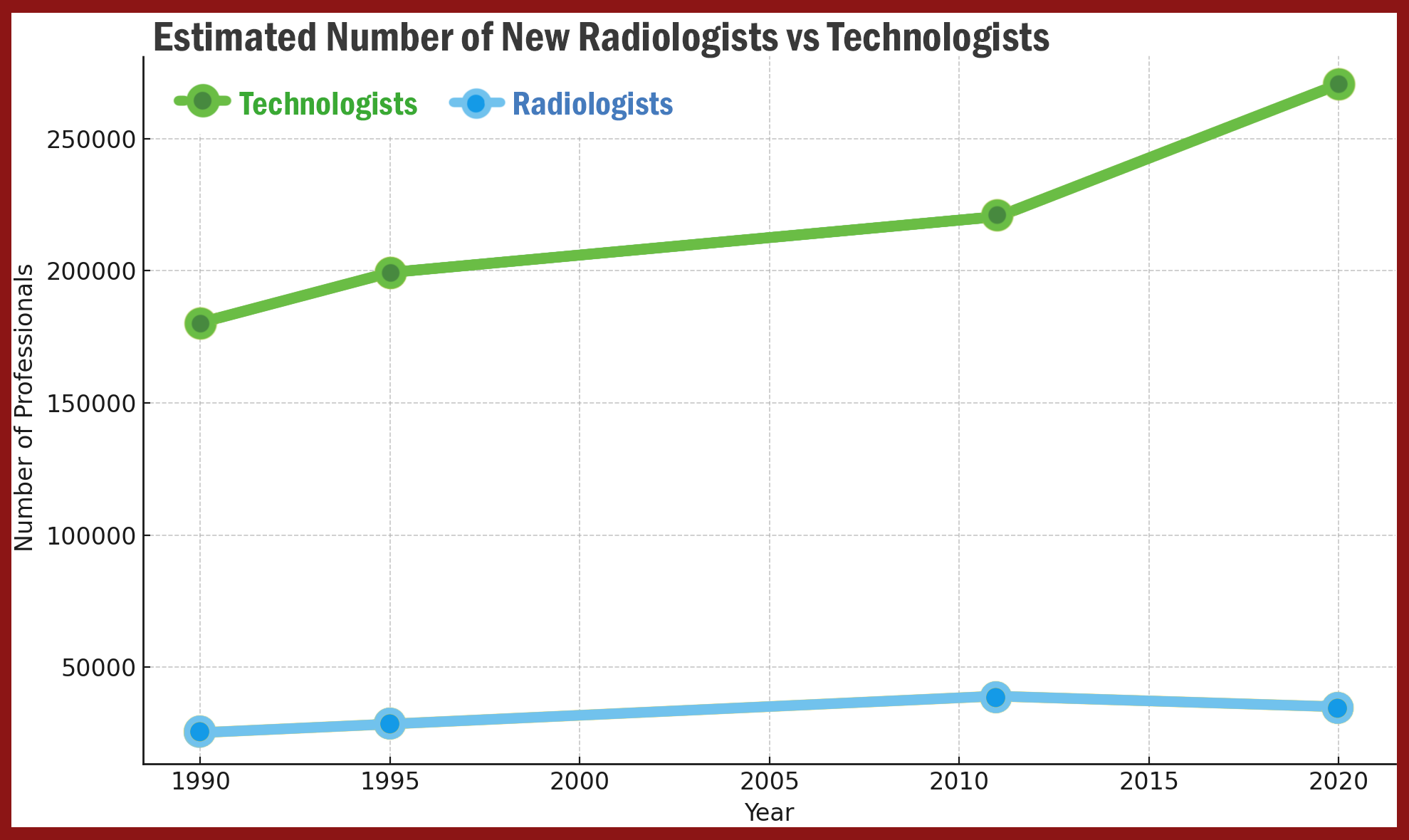
Figure F: Output of techs vs radios.
Clinical Impact and Return on Investment
The work produced by a 3D lab directly supports clinical decision-making. This can lead to more precise procedures, shorter operative times, and fewer complications. In some cases, this insight may even help avoid unnecessary surgeries. These benefits often translate into measurable savings. Fewer complications mean fewer reoperations, shorter operating room times, and reduced hospital stays. While not every case delivers a direct financial return, the cumulative impact across a high-volume institution can be significant. By improving outcomes and reducing inefficiencies, a 3D lab contributes to both better care and a more sustainable health system.
Figure F: Impact on community, and marketing for institution blurb.


