What is DIEP Flap Reconstruction?
The DIEP flap is a breast reconstruction technique that uses a flap of skin and fat from the lower abdomen, along with its supplying blood vessels, to create a new breast after mastectomy. Unlike older methods, it leaves the abdominal muscles intact—only the tissue needed for reconstruction is removed. This reduces the risk of long-term weakness or hernia. The DIEP flap is a strong option for patients who want a more natural result, have enough abdominal tissue, and prefer to avoid implants. Because the transferred tissue must stay well-perfused to survive, identifying the most reliable blood vessels before surgery is essential.
Learn more about the DIEP flap procedure here: https://www.breastcancer.org/
Figure A (Right): 3D rendering of the abdominal region where perforators are harvested. The abdominal muscles and umbilicus are shown in transparent blue, with perforating vessels highlighted in pink.
3D Imaging
3D imaging can play an important role in supporting DIEP flap breast reconstruction by helping surgeons visualize critical anatomy before the procedure. A CT angiogram of the abdomen is performed to capture detailed images of the abdominal wall, with intravenous contrast used to highlight blood vessels. From this scan, radiologic technologists segment the deep inferior epigastric arteries and their perforating branches which supply blood to the flap tissue (these vessels exit the abdominal wall and reach into the belly fat). The umbilicus is segmented as a landmark, and the rectus abdominis muscle (ab muscle) is included to show the course of the vessels through the muscle layer. This mapping allows surgeons to identify the most favorable perforators and understand their spatial relationships, which vary from patient to patient. The segmented data is then sent to clinicians through the hospital’s PACS system, providing a digital reference for preoperative review and planning.
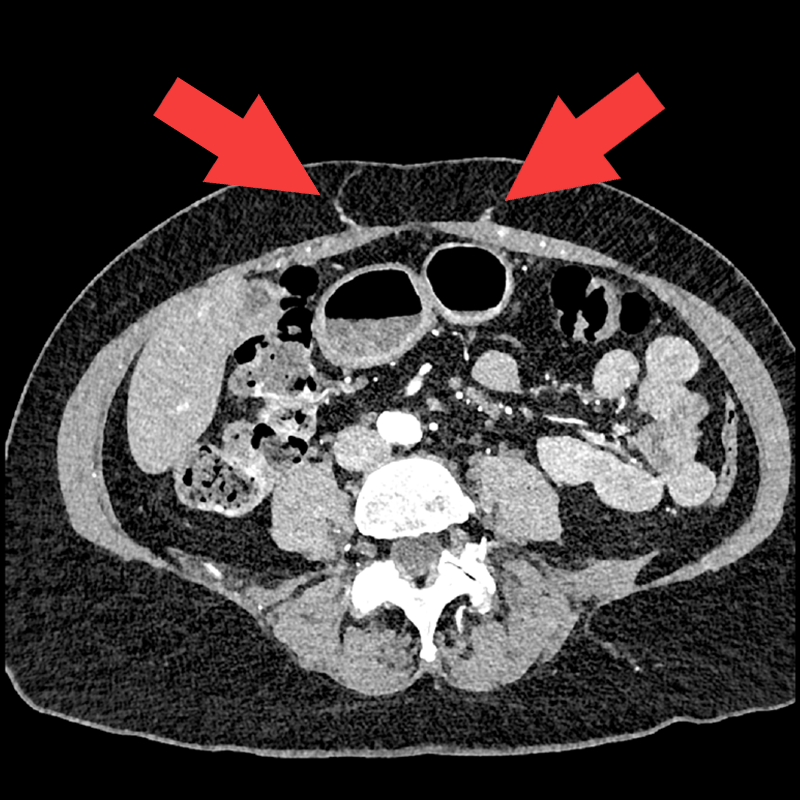
Figure B: Axial imaging of the abdomen with arrows pointing to perforating vessels that might be used for flap reconstruction.
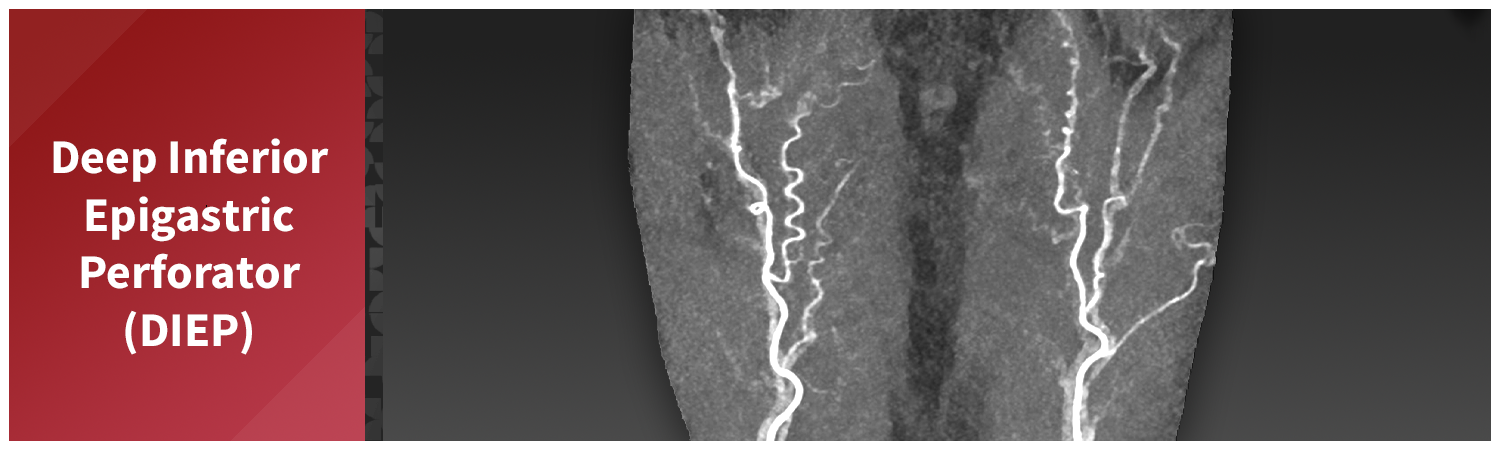
Figure C: Rotating segmented MIP image of the abdomen, provided to clinicians for preoperative evaluation and planning.
Figure D: Rotating 3D volume render is also provided to the clinician via the hospital’s PACS system.
3D Printing
In addition to the 3D imaging provided to the clinicians, a 3D mesh file is exported by the quality control technologist and passed to our 3D printing team for further design and fabrication. The physical model shows the perforators in context with the rectus muscle and umbilicus, providing a tactile and spatial reference during preoperative planning. The 3DQ Lab developed the 3D print design in close collaboration with the surgeons who use these prints, evolving through multiple iterations before settling on a design that optimally aligned with surgical needs.
Clinicians often bring the model with them into the operating room, where it serves as a real-time reference during reconstruction. They may either prop up the model outside of the sterile field or put the model in a sterile bag so they can handle it during surgery. These models support perforator selection, flap design, and may help reduce operative time and improve surgical confidence.
Figure E: Design steps are taken by our 3D printing team to prepare for fabrication.
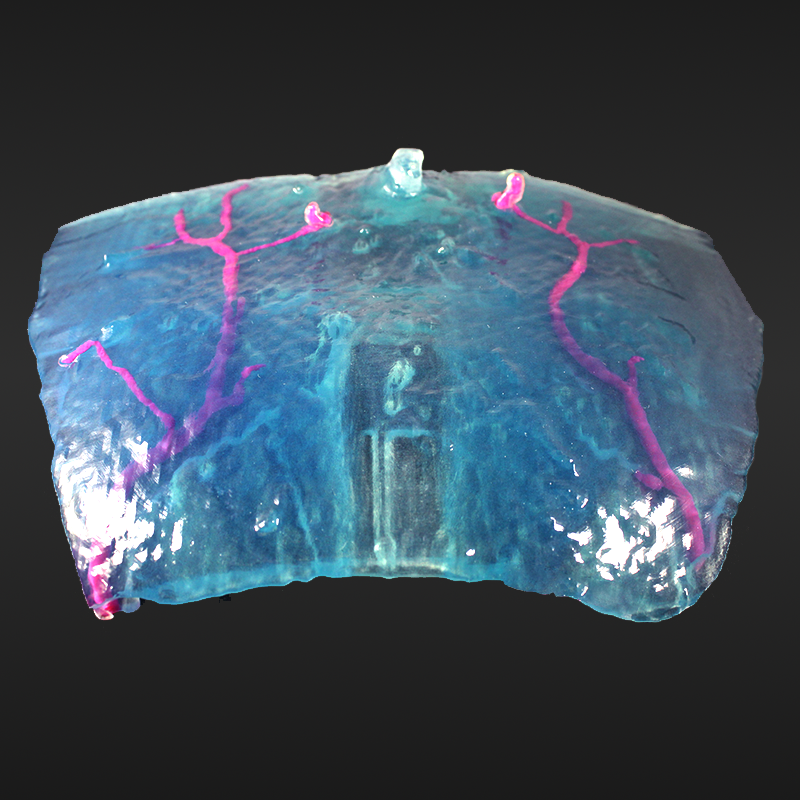
Figure F: 3D printed model based on segmented data. The rectus muscle and umbilicus are shown in transparent blue, with perforating arteries highlighted in magenta.

