An asymptomatic patient with an aortic aneurysm was referred to the 3DQ Lab for aortic surveillance. This program tracks changes in aortic size over time, with measurements plotted on a graph. Because each segment of the aorta has its own surgical threshold, he cardiothoracic surgery team uses this data to identify the critical window for intervention, preventing rupture while also avoiding surgery before it becomes necessary. (Learn more about Aortic Surveillance here).
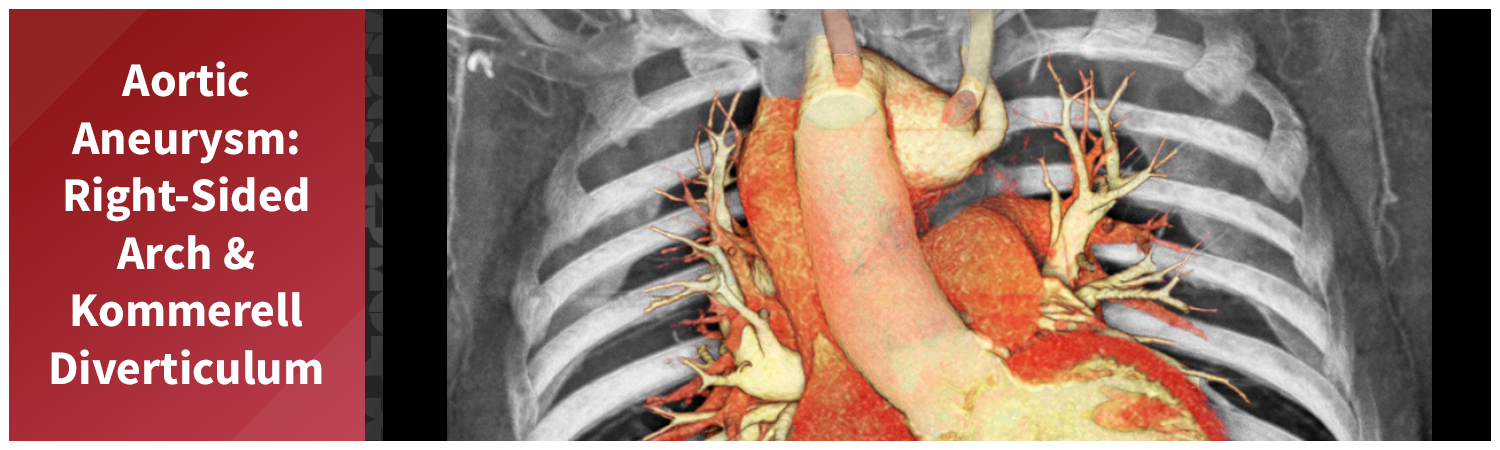
This case, however, involved unusual anatomy. The patient had a right-sided aortic arch, a congenital anomaly in which the aorta curves to the right side of the chest instead of the left. The branching pattern was also atypical. The first branch from this patient’s arch was the left common carotid artery, followed by the right common carotid and right subclavian arteries. The final branch was an aberrant left subclavian artery, which arose from a large Kommerell diverticulum, an outpouching often associated with arch anomalies. The descending thoracic aorta was tortuous, with an aneurysm identified at its proximal portion.
Figure A (Right): 4D rotational volume render of the heart and thoracic aorta, showing the arch branching pattern, Kommerell diverticulum, and proximal descending aneurysm. (Learn more about 4D/ time resolved imaging here).
A gated CT angiography of the chest was obtained to generate the images and measurements needed for aortic surveillance. This scan was the most recent in a series of follow-up studies since the patient was first identified with an aortic aneurysm and arch anomalies. The aortic surveillance program relies on these regularly scheduled scans to track changes over time. Measuring data over time is part of a process known as longitudinal analysis, learn more here. In this case, the Kommerell diverticulum has maintained a mostly consistent size over time, while the proximal aortic aneurysm has shown measurable enlargement.
Figure B: 4D axial cut-plane volume rendering of the thoracic aorta and heart, with the plane moving in the axial direction to demonstrate internal anatomy.
Figure C: 4D coronal cut-plane volume rendering of the thoracic aorta and heart, with the plane moving in the coronal direction to demonstrate internal anatomy.
Figure D: 4D sagittal cut-plane volume rendering of the thoracic aorta and heart, with the plane moving in the sagittal direction to demonstrate internal anatomy.
A 3DQ Lab technologist processed the scan using our aortic surveillance protocol. Standardized measurements were taken at set locations along the aorta to ensure consistency with prior studies. Volume-rendered images were generated to visualize the morphology of the aorta and its branch vessels in three dimensions. Curved planar reformats of the coronary arteries were also created to assess their course and relationship to the aortic anatomy. All measurements were then added to the patient’s graph alongside those from previous visits, demonstrating how the size of the aorta has changed over time. Below are the images provided to the Cardiothoracic Surgery team.
Figure E (Right): Measurements from this patient are plotted on a graph to show how aortic diameters at specific locations have changed over time. This helps visualize trends and provides a clear picture of the aorta’s overall health and progression.
Figure F: Standardized aortic diameter measurements obtained at predetermined locations along the thoracic aorta for surveillance.
Figure G: Targeted volume renderings of the heart, thoracic aorta, and coronary arteries for visualization of anatomy and vessel morphology. (Learn more about volume renders here).
Figure H: Curved planar reformats (CPRs) showing the course of the coronary arteries and their relationship to the thoracic aorta. (Learn more about CPRs here).

